

When a breast cancer diagnosis lands, most people do what feels instinctive: they Google the biggest hospital name they know, call the most advertised number, and show up wherever the first available appointment is. That instinct isn’t always wrong, but it isn’t always right either. The right breast cancer treatment hospital in Hyderabad isn’t necessarily the biggest or the most advertised. It’s the one with the right surgical team, the right infrastructure, and a support system built around your specific diagnosis and stage.
The stakes here are real. The hospital you choose determines not just your treatment plan but your recovery, your long-term outcomes, and how much of the entire process you understand and control as a patient. A general hospital that “also does cancer” is a very different environment from a dedicated breast oncology centre where the nursing staff have seen hundreds of post-operative mastectomy patients and the surgical team reviews every case before the first incision. That difference shows up in outcomes. It shows up in how complications are caught. And it shows up in how you feel walking out of a consultation, whether you understood what was said or left more confused than when you walked in.
Dedicated breast cancer care centres in Hyderabad exist specifically because that gap is real. Patients travel from across Telangana and Andhra Pradesh to hospitals with dedicated breast surgery and gynae oncology departments led by senior specialists, not generalists rotating through oncology. Asvins Specialty Hospitals is one such centre. By the end of this guide, you will have a concrete framework for evaluating any breast cancer hospital in Hyderabad, a shortlist of centres worth considering, the cost ranges to plan around, and the specific questions to ask before you agree to anything.
What Separates a Genuine Breast Oncology Centre from a General Hospital
Most hospitals in Hyderabad will tell you they treat breast cancer. Fewer have the infrastructure to back that claim up. There is a meaningful difference between a hospital that handles breast cancer cases among hundreds of other procedures and a centre built around breast oncology as a primary specialty. That difference matters more than most patients realise when they are first searching.
Dedicated Departments vs. General Oncology Wards
A hospital with a standalone breast surgery unit provides a different standard of care for one simple reason: the entire environment is calibrated for it. The surgical protocols are specific to breast oncology. Case volume is higher, which means the nursing staff understand post-operative breast surgical care in detail, not as a variation of general post-surgical recovery. Complication patterns are recognised earlier because the team has seen them repeatedly. In a general oncology ward where breast cases are mixed with colorectal, head and neck, and lung surgeries, that depth of familiarity is harder to maintain.
Case volume matters because surgical skill in oncology is cumulative. High-volume breast surgeons, those who perform a substantial proportion of breast cases each year, develop faster, more refined decision-making around margins, sentinel node assessment, and reconstruction options than surgeons who handle breast cases occasionally within a broader general surgical mix. This is not an abstract point. It has direct consequences for whether you need a second surgery to achieve clear margins and how your recovery unfolds.
Accreditation Markers Worth Checking
NABH (National Accreditation Board for Hospitals and Healthcare Providers) and JCI (Joint Commission International) accreditations are basic quality signals worth verifying. In practical terms, accreditation means the hospital has been evaluated against standardised protocols for medication safety, infection control, surgical safety, clinical documentation, and staff competence. For cancer patients specifically, this matters because chemotherapy administration, radiation safety, and surgical oncology workflows each carry serious risks when systems are poorly managed.
NABH requires hospitals to demonstrate compliance across evaluated criteria, with audited quality improvement systems. JCI goes further with international patient safety goals covering accurate patient identification, safe medication handling, and care coordination across specialties. Neither accreditation guarantees the best outcome for every patient, but the absence of either should prompt a direct question: what quality framework does this hospital follow? A hospital that cannot answer that clearly is one worth being cautious about.
Multidisciplinary Tumour Boards and Why They Change Outcomes
A tumour board is a regular meeting where a surgical oncologist, medical oncologist, radiation oncologist, pathologist, and radiologist review each case together before a treatment plan is finalised. This is not a procedural formality. Research consistently shows that multidisciplinary tumour board review leads to more comprehensive planning and frequently changes or refines treatment recommendations compared with single-specialist decisions. Research on multidisciplinary tumour boards supports the idea that
team-based review materially affects treatment choices. A stage 2 tumour that looks straightforward on first review might have molecular features that shift the recommendation from surgery-first to neoadjuvant chemotherapy followed by surgery.
A breast cancer treatment hospital in Hyderabad that treats patients without a functioning multidisciplinary tumour board as standard practice is missing a critical safety layer. Ask any prospective hospital directly: is tumour board review standard for every breast cancer patient, or is it reserved for
complex cases? The answer tells you a great deal about how seriously the institution approaches clinical decision-making.
Surgical Options Every Patient Should Understand Before Their First Consultation
Walking into a breast surgery consultation without understanding the basic surgical options leaves you entirely dependent on what you are told, without any framework to evaluate it. You don’t need a medical degree. But you do need to understand what is being proposed, why, and what the alternatives are. That knowledge is the difference between informed consent and passive agreement.
Lumpectomy: When Breast Conservation Is the Right Call
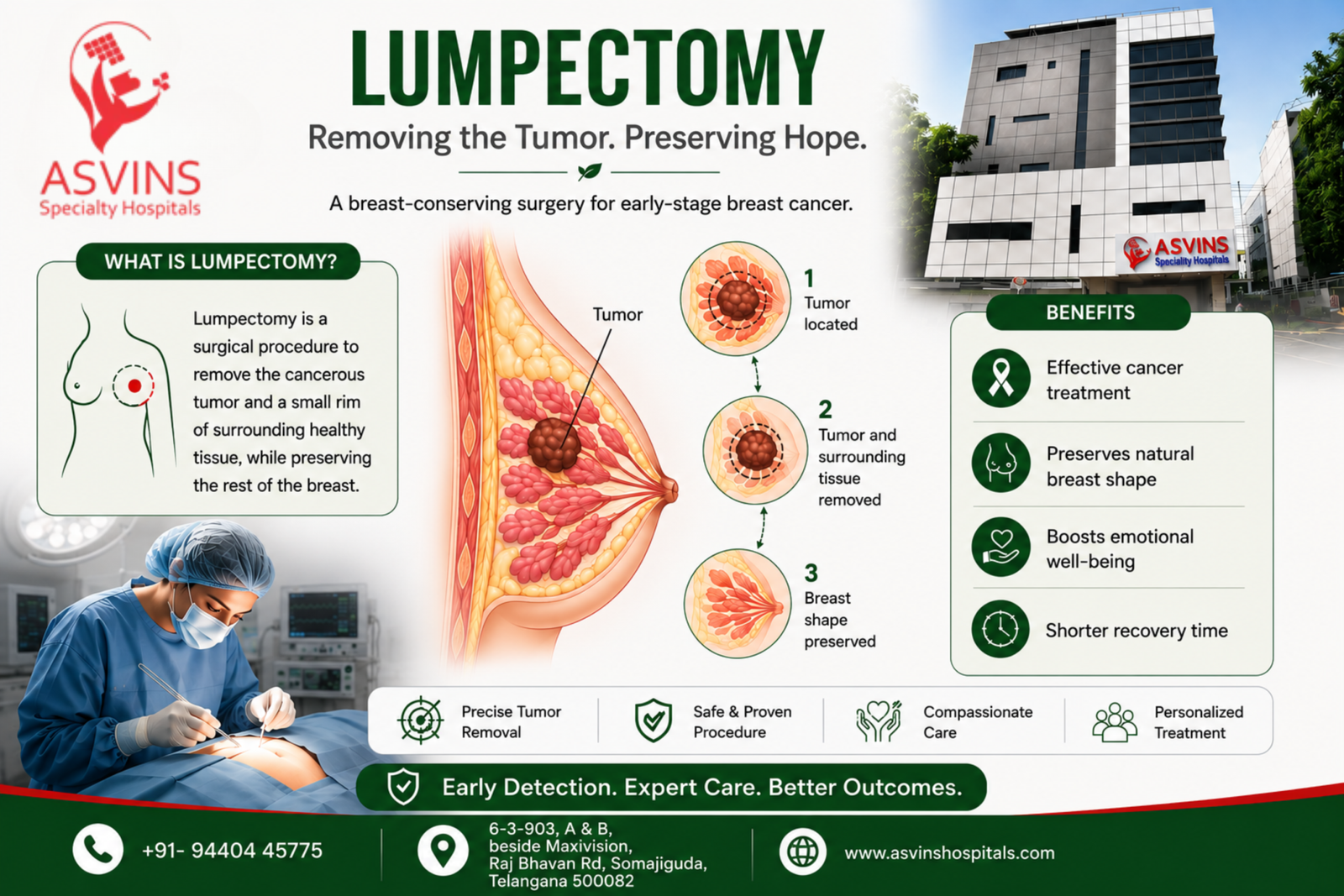
A lumpectomy removes the tumour and a surrounding margin of healthy tissue, leaving the rest of the breast intact. It is the surgical option for early-stage breast cancer with smaller tumours in favourable locations, where clear margins can be achieved while preserving the breast. The procedure is almost always followed by radiation therapy, which is part of why long-term survival outcomes for lumpectomy plus radiation are comparable to mastectomy in eligible patients.
The common misconception is that “smaller surgery means less effective treatment.” This is not accurate. For an early-stage tumour with no genetic risk factors and a favourable tumour-to-breast-size ratio, lumpectomy is not a compromise, it is the clinically appropriate choice. For a practical comparison when deciding on surgical approach, see choosing between mastectomy and lumpectomy. The key question is whether your tumour location, size, and biology make you a good candidate, and that requires a surgeon who evaluates each case individually rather than defaulting to one approach.
Mastectomy: What It Involves and When Surgeons Recommend It
Mastectomy removes the entire breast. A simple mastectomy removes the breast tissue and nipple. A modified radical mastectomy also removes the axillary lymph nodes. The surgical recommendation shifts toward mastectomy when the tumour is large relative to breast volume, when there are multiple tumours in different parts of the breast, when the patient carries a BRCA1 or BRCA2 genetic mutation, when the cancer is inflammatory, or when the patient has had prior chest radiation that makes further radiation after lumpectomy unsafe. Patient preference, after full counselling on both options, is also a legitimate factor in the final decision.
Mastectomy means longer recovery, greater immediate surgical impact, and reconstruction decisions that lumpectomy does not require. But for the right patient and the right tumour, it is not the more aggressive option, it is the correct one. Any surgeon who cannot clearly explain why they are recommending mastectomy over lumpectomy, or lumpectomy over mastectomy, in the context of your specific diagnosis and imaging, is not meeting the standard you should expect from a breast oncologist.
Oncoplastic Techniques and Reconstruction: Questions Worth Asking
Oncoplastic surgery combines tumour removal with plastic surgery approaches to preserve or restore breast shape at the same time. For patients undergoing lumpectomy, this can mean reshaping the remaining tissue so that the cosmetic outcome is significantly better than a standard partial removal. For mastectomy patients, reconstruction can be performed using implants or the patient’s own tissue from the back, abdomen, or thigh, either immediately at the time of mastectomy or as a planned second procedure.
Not every breast cancer treatment hospital in Hyderabad has oncoplastic capability within the same surgical team. Some hospitals perform the cancer surgery and then refer reconstruction to a separate facility. Ask the hospital directly: is oncoplastic or reconstructive surgery performed by the same team that does the cancer surgery, or is it referred out? The answer affects the continuity of your care and the coordination of your surgical plan.
Chemotherapy Protocols: What a Strong Breast Cancer Programme Looks Like
Not every breast cancer diagnosis leads to chemotherapy. Hormone receptor-positive, early-stage cancers in older patients may require surgery and hormonal therapy alone. But when chemotherapy is part of the plan, the quality of the programme around it matters enormously. Knowing what a strong breast cancer chemotherapy service looks like helps you evaluate what you are being offered.
Standard Regimens Used in Breast Cancer Treatment
In 2026, the most commonly used chemotherapy backbone for breast cancer is AC-T: doxorubicin (Adriamycin) and cyclophosphamide, followed by a taxane such as paclitaxel or docetaxel. Dose-dense AC-T delivers the same drugs at shorter intervals, typically every two weeks instead of three, using growth factor support to manage blood count recovery. This approach is used for higher-risk early breast cancer where more intensive treatment is clinically justified. CMF (cyclophosphamide, methotrexate, fluorouracil) is an older regimen still used in selected cases where anthracyclines or taxanes are not suitable for a particular patient.
The terms “neoadjuvant” and “adjuvant” come up in almost every treatment discussion. Neoadjuvant chemotherapy is given before surgery, with the goal of shrinking the tumour to make surgery more feasible or to make breast conservation possible in cases where mastectomy would otherwise be required. Adjuvant chemotherapy is given after surgery to reduce the risk of recurrence. Understanding which you are being prescribed, and why, is a basic piece of information you are entitled to at every
consultation.
Targeted Therapy and Hormone Therapy: When They Apply

HER2-positive breast cancers respond to targeted therapy using trastuzumab (Herceptin), often combined with pertuzumab, alongside standard chemotherapy. Hormone receptor-positive cancers, the most common subtype, are typically managed with hormonal therapy: tamoxifen for premenopausal women and aromatase inhibitors such as anastrozole or letrozole for postmenopausal women. These are not optional add-ons. For the right subtype, they are central to the treatment plan and significantly reduce recurrence risk.
Not all hospital pharmacy and infusion units are equipped to administer targeted therapies safely. The storage, preparation, and administration of agents like trastuzumab require trained oncology pharmacy staff and proper cold chain management, in line with oncology pharmacy best practice guidelines. Before choosing a hospital, confirm that the oncology pharmacy can support the full regimen your subtype requires. This is a basic infrastructure question worth asking directly.
What a Proper Chemotherapy Unit Looks Like
A proper chemotherapy infusion unit has dedicated infusion chairs in a clean, monitored space, with oncology-trained nursing staff present throughout every infusion session. Antiemetic protocols, hydration support, and monitoring for infusion reactions are standard. Same-day emergency access for chemotherapy-related complications is not optional: severe neutropenia, fever, hypersensitivity reactions, or signs of infection require immediate clinical attention, not a scheduled appointment the following week.
These are not luxury features, they are baseline requirements for safe systemic cancer treatment. A hospital that cannot describe its chemotherapy monitoring and emergency protocol clearly is one where the infrastructure around systemic treatment has not been built out properly, regardless of what the brochure says.
How to Evaluate a Breast Surgeon’s Credentials Without Getting Lost in Titles
The string of letters after a surgeon’s name in India, MBBS, MS, MCh, DNB, FRCS, tells you something about training, but it doesn’t tell you everything about the surgeon’s actual focus, case volume, or subspecialty depth. Learning to read credentials in the context of breast oncology specifically is worth a few minutes of your time before you commit to a consultation.
The Qualifications That Actually Matter in Surgical Oncology
MCh (Surgical Oncology) or DNB (Surgical Oncology) represents the highest formal training qualification for a surgical oncologist in India. These are postgraduate superspecialty degrees that require a minimum of three years of dedicated surgical oncology training after MS (General Surgery). A general surgeon or gynaecologist without subspecialty oncology training is not the same clinical entity as a trained surgical oncologist, regardless of hospital affiliation or the department name on the hospital website.
This distinction matters in breast cancer because surgical oncologists are trained specifically in oncological principles of resection: margin assessment, lymph node management, sentinel node biopsy technique, and the integration of surgical decisions with the broader multimodal treatment plan. A skilled general surgeon may perform technically clean operations. The oncological decision-making layer, however, requires subspecialty training that general surgery alone does not provide.
Experience, Caseload, and Specialisation: What to Ask Directly
Years of experience matter most when they are concentrated in breast oncology specifically, not spread across general oncology or general surgery. A surgeon whose career has focused on breast oncology builds a different level of subspecialty depth than one who handles breast cases within a wider surgical mix that includes head and neck, colorectal, and thoracic cases. Both may be competent surgeons. They are not equivalent in breast-specific experience.
Ask directly during the consultation: how many breast surgeries does the operating surgeon perform per year? What proportion of the surgeon’s practice is breast surgery specifically? Has the surgeon published or presented in the field of breast oncology? These are reasonable questions. A surgeon with genuine depth in this area will answer them without hesitation.
Notable Surgical Oncologists in Hyderabad for Breast Cancer Treatment
Dr. Digumarti Raghunadharao brings over 45 years of experience in surgical oncology, with expertise across breast, head and neck, GI, and gynaecological cancers. A team of dedicated surgical oncologists, including Dr. G Ramani and colleagues, handles high volumes of breast cancer surgery within a non-profit model.
At Asvins Specialty Hospitals, Dr. G. Suryanarayana Raju brings over 40 years of specialised oncology experience and is the founder of the Surgical Oncology Department at NIMS Hyderabad. That founding role, at one of India’s premier public oncology institutions, reflects a career concentrated in dedicated surgical oncology at an institutional level that shapes the clinical programme at Asvins today.
Choosing a Breast Cancer Treatment Hospital in Hyderabad: The Shortlist

Several hospitals in Hyderabad are capable of treating breast cancer. The differentiator between them is the depth of specialisation, the seniority of the operating team, and the continuity of care built around each patient. Here is an honest overview of the centres worth knowing about.
Asvins Specialty Hospitals: Dedicated Breast Surgery and Gynae Oncology Under One Roof
Asvins operates as a specialist cancer hospital rather than a large general multi-specialty facility. The breast surgery and gynae oncology departments are led by senior specialists, with Dr. G. Suryanarayana Raju’s four-decade track record in surgical oncology as the clinical foundation. His background as the founder of the Surgical Oncology Department at NIMS, a government institution known for training India’s surgical oncologists, means the expertise at Asvins reflects senior-level, high-volume oncology practice delivered in a private specialist setting with personalised attention.
The hospital offers comprehensive oncology services including surgical oncology, medical oncology, gynae oncology, thoracic oncology, and haematology, with full hospital infrastructure: ICU, OT, CT scan, dialysis, X-ray, ultrasound, 24/7 laboratory, pharmacy, and ambulance services. For a breast cancer patient, this means the diagnostic workup, surgery, systemic treatment, and follow-up care can all be managed within one coordinated environment, without being transferred between facilities at each stage of the treatment pathway. That continuity reduces the coordination failures that affect patient care when treatment is fragmented across multiple hospitals, and it is one of the clearest reasons patients seek out dedicated breast cancer care centres rather than large general institutions.
Other Reputable Centres Worth Knowing
One facility in Secunderabad is South Asia’s first free-standing comprehensive breast health centre. As a purpose-built breast-focused facility, it provides a high level of specialist attention, with multidisciplinary breast care as its central function. Another major centre in Jubilee Hills offers oncoplastic breast surgery, robotic surgery, and advanced imaging including tomosynthesis, supported by a large multi-specialty infrastructure. The scale of this operation comes with the trade-off that oncology is one of many large departments within a major corporate hospital system.
A non-profit, high-volume cancer centre in Banjara Hills operates with particular strength in affordability and breadth of oncology services, including genetic counselling for breast cancer patients. Another facility in the same area focuses on modern systemic therapies, offering targeted therapy, immunotherapy, and advanced radiotherapy alongside breast-conserving surgery and reconstruction options. A separate hospital provides sentinel node biopsy, axillary lymph node dissection, and structured surgical protocols, with treatment decisions driven by tumour biology, stage, hormone sensitivity, and patient fitness.
What to Watch for When Hospitals Make Claims
Many hospital websites in Hyderabad list every possible cancer treatment as “available” without specifying caseload, team seniority, or clinical outcomes. The presence of a technology on a capability list and the routine, experienced use of that technology in patient care are two different things. A hospital that lists oncoplastic surgery on its website but refers that work to a separate plastic surgery team, or performs it rarely, offers a meaningfully different experience than one where the breast surgical team integrates oncoplastic techniques as standard for every eligible case.
Before registering at any hospital, ask for case volumes, request to meet the actual operating surgeon before admission rather than a junior team member, and confirm that multidisciplinary tumour board review is standard for every breast cancer case from the start. Hospitals that hesitate to answer these questions directly are telling you something important about how they operate.
Breast Cancer Treatment Cost in Hyderabad: What the Numbers Actually Look Like
Cost is a real factor in every family’s decision, and pretending otherwise does not help anyone plan effectively. The following figures are realistic estimates based on current data for Hyderabad hospitals. They are ranges, not fixed prices, because actual costs depend on stage, hospital tier, room category, and the specific regimen your treatment plan requires.
Cost by Procedure
For surgical treatment, lumpectomy in Hyderabad typically costs between INR 1,56,000 and INR 2,14,000. Mastectomy ranges from approximately INR 1,50,000 to INR 4,00,000 depending on the extent of the procedure, whether lymph node dissection is included, and the hospital’s pricing structure. Breast reconstruction, if planned, adds a substantial further cost beyond the mastectomy base price and varies widely based on whether implant-based or tissue-based reconstruction is chosen.
Chemotherapy cycles are priced between approximately INR 50,000 and INR 2,00,000 per cycle, with the wide range reflecting the difference between standard regimens and targeted therapy combinations.
Radiation therapy runs from approximately INR 20,000 to INR 75,000 per course. Targeted therapy sessions, such as trastuzumab infusions for HER2-positive disease, can run to INR 90,000 or more per session. For a complete multimodal treatment plan covering surgery, multiple chemotherapy cycles, radiation, and targeted therapy, total cost across the full plan in Hyderabad can range from INR 3 lakh to INR 15 lakh or more depending on stage and regimen complexity.
Stage-Based Cost Context
A Stage 1 breast cancer diagnosis treated with lumpectomy followed by radiation and possibly hormonal therapy looks very different in cost from a Stage 3 diagnosis requiring neoadjuvant chemotherapy,
modified radical mastectomy, adjuvant chemotherapy, radiation, and targeted therapy. Stage 1 surgical plans often stay within the INR 1.5 to 3 lakh range when treatment is surgery and radiation alone. Stage 2 and 3 plans that require multiple chemotherapy cycles on top of surgery and radiation can reach INR 8 to 15 lakh or beyond, depending on the specific regimen and whether targeted agents are part of the plan. Stage 4 disease, where the goal shifts to disease control rather than cure, is a different financial and clinical conversation entirely.
Insurance, Government Schemes, and Financial Counselling
Ayushman Bharat/PMJAY provides coverage for qualifying patients across a range of cancer treatment procedures. If you or your family member qualifies based on income and registration status, verify with the hospital’s admissions team whether your planned procedure is covered under the scheme before treatment begins. Private health insurance policies vary considerably in how they cover cancer treatment: some provide comprehensive oncology coverage including chemotherapy, while others exclude certain treatments or cap payouts in ways that only become clear when a claim is filed.
Ask any hospital you are considering whether they have a dedicated financial counsellor or social welfare officer who can walk through your insurance situation, available government schemes, and EMI options before you commit to treatment. A hospital that has this service embedded in its patient pathway is investing in helping patients navigate cost in a structured way, and that matters when treatment runs across months and financial planning becomes part of the recovery process.
The Patient Pathway from Diagnosis to First Treatment
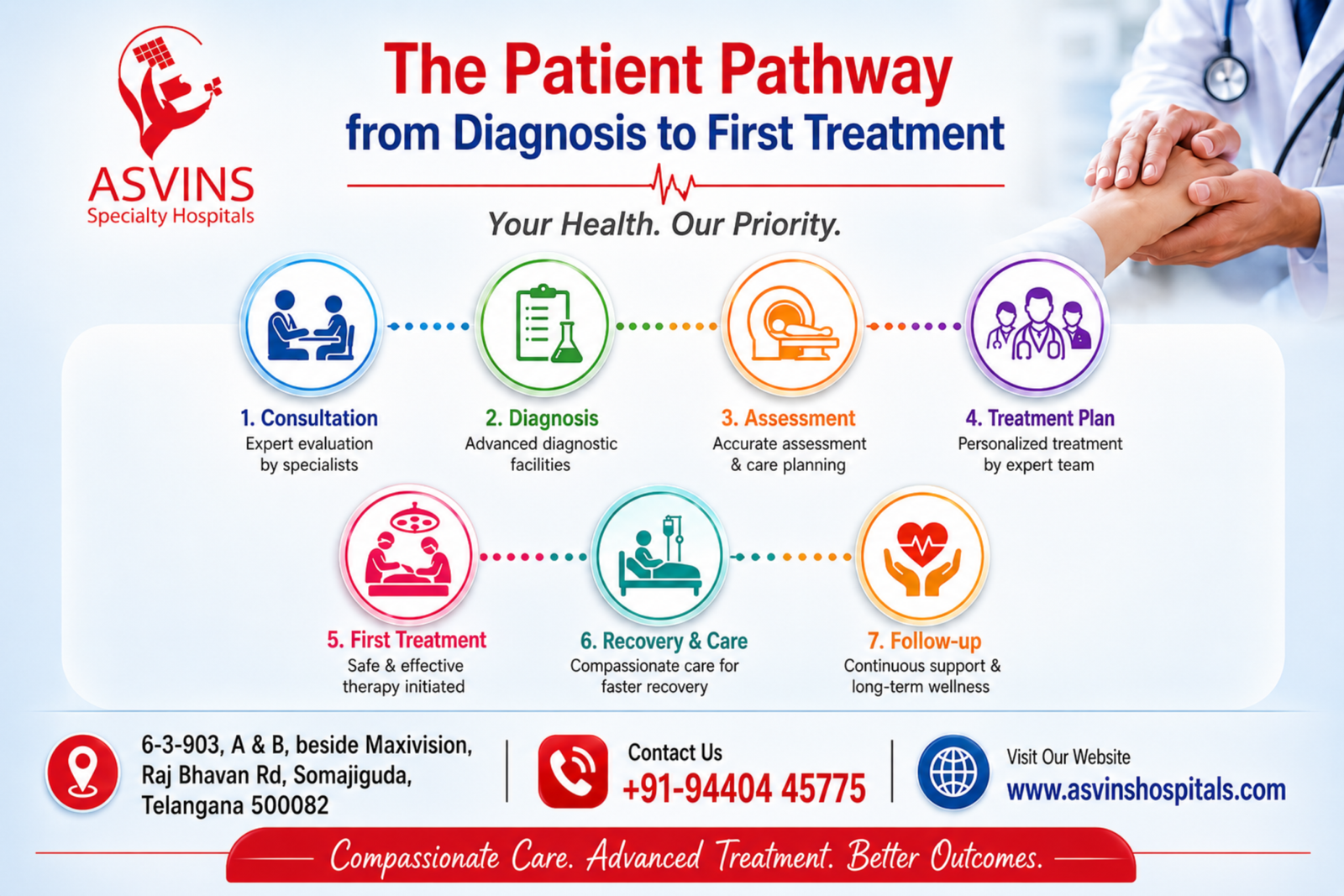
One of the most anxiety-inducing aspects of a new breast cancer diagnosis is not knowing what happens next and how long the process takes before treatment starts. The sequence is more predictable than it feels in the first week after diagnosis. Understanding it helps you move through it with more clarity and less panic.
Typical Timeline from Biopsy to Treatment Start
Biopsy results typically take 2 to 7 days, sometimes longer if special staining for hormone receptor or HER2 status is needed. Staging workup including CT scan, MRI, or PET scan runs from same-day to one week, depending on scheduling and urgency. Specialist consultation and tumour board review generally happen within a few days to one week of receiving biopsy results at a well-organised hospital. Preoperative evaluation, covering blood tests, ECG, anaesthesia assessment, and cardiology clearance for older patients, adds 1 to 7 days depending on findings. From confirmed diagnosis to treatment start, a well-functioning breast cancer treatment hospital in Hyderabad moves most patients into treatment within 1 to 3 weeks.
Factors that extend this timeline include: the need for a repeat biopsy if initial sampling was inadequate,
incomplete pathology due to laboratory turnaround, insurance authorisation delays, PET/CT scheduling backlogs, and the patient’s decision to seek a second opinion before committing to a treatment plan.
None of these delays, when managed actively, push treatment to a point where outcomes are meaningfully compromised in most early and locally advanced cases. The one situation where urgency is higher is inflammatory breast cancer, which moves faster clinically and requires faster action.
Pre-Operative Evaluation and Genetic Testing
Standard pre-operative workup covers complete blood count, kidney and liver function tests, ECG, and anaesthesia clearance. Older patients or those with cardiovascular history require cardiology evaluation before surgery is scheduled. For breast cancer specifically, BRCA1 and BRCA2 genetic testing is available at larger Hyderabad centres and through specialised pathology labs. Simple marker testing typically returns in a few days. Larger next-generation sequencing panels take 1 to 3 weeks.
BRCA results have direct consequences for surgical decisions. A BRCA1 or BRCA2 positive result in a premenopausal patient with breast cancer substantially changes the risk calculus around lumpectomy versus mastectomy, and may also raise the question of contralateral risk-reduction mastectomy. Knowing your BRCA status before finalising a surgical plan is genuinely important for the right patient, not a detail to be addressed after surgery has already been scheduled. Ask your surgeon directly whether BRCA testing is relevant to your case before the surgical plan is locked in.
Getting a Second Opinion Without Losing Critical Time
A second opinion from a senior specialist before committing to a surgical plan is medically sound and does not meaningfully delay treatment in the vast majority of breast cancer cases. The window between diagnosis and surgery in early to locally advanced breast cancer is not so narrow that a week spent getting a senior oncologist to review your pathology slides, imaging, and receptor status compromises your outcome. What you bring to a second-opinion consultation determines how useful it is: biopsy report, pathology slides (not just a summary), imaging CDs, receptor status (ER, PR, HER2), and any staging scan results already completed.
A second opinion is particularly worth pursuing when the diagnosis is unclear, when the proposed treatment plan feels inconsistent with what you have read or been told elsewhere, when a young woman is being offered mastectomy without discussion of genetic testing, or when the treatment recommendation comes from a generalist rather than a trained surgical oncologist. At Asvins Specialty Hospitals, senior specialist consultations are available for patients who have already received a treatment plan elsewhere and want an experienced oncology review before proceeding.
Patient Support Services That Separate Good Hospitals from Great Ones
Treatment does not begin and end in the operating room or the infusion chair. How a hospital supports patients through diagnosis, surgery, chemotherapy, and recovery, the months that span the full treatment arc, determines the real quality of the patient experience. These services are worth asking about explicitly before you register anywhere.
Psychological Counselling and Patient Navigation
Clinical studies on psychosocial interventions in oncology consistently show that breast cancer patients who receive structured psychological support report better treatment adherence, lower anxiety and distress scores, and stronger overall recovery outcomes. Hospitals that embed a counsellor or social worker within the oncology team, rather than offering a referral list on request, produce a meaningfully different patient experience. The counsellor knows the treatment team, understands the treatment timeline, and can intervene proactively when a patient’s mental health is affecting their ability to complete chemotherapy or attend follow-up appointments. Evidence and patient advocacy groups note that supportive care improves quality of life for metastatic breast cancer patients, illustrating the value of integrated psychosocial services.
Patient navigation is equally important. A nurse navigator or care coordinator who tracks your treatment plan, follows up on test results, and connects you with the right team member when a problem arises removes an enormous amount of coordination burden from patients and families during an already overwhelming period. Ask any hospital: do you have a patient navigator or coordinator assigned to oncology patients, or do patients manage their own care coordination between departments?
Nutritional Guidance During Chemotherapy and Recovery
Chemotherapy affects appetite, taste, and gastrointestinal function in ways that differ from other illnesses, and the specific effects vary by regimen. AC-T causes nausea and appetite suppression in most patients. Dose-dense regimens accelerate those effects. Taxane-based chemotherapy causes neuropathy that can affect a patient’s ability to prepare food or maintain normal dietary habits. A clinical dietitian with oncology-specific experience can make a real difference in a patient’s ability to maintain adequate nutrition through treatment, which in turn affects treatment tolerance and recovery.
A hospital with an in-house oncology dietitian is a meaningful differentiator from one that offers generic dietary advice or refers patients to a general nutritionist unfamiliar with the specific demands of systemic cancer treatment. When evaluating hospitals, ask specifically whether there is an oncology-trained dietitian on staff, not just a general nutrition consultation service available somewhere in the building.
Post-Treatment Follow-Up and Survivorship Planning
Surveillance after breast cancer treatment follows a structured schedule: clinical breast examination every 3 to 6 months for the first three years, annual mammography of the remaining or reconstructed
breast, and regular blood marker testing where indicated. A hospital that builds this follow-up into a structured survivorship programme monitors for recurrence systematically and manages late treatment effects, lymphoedema, cardiac monitoring for patients who received anthracyclines, bone density management for patients on aromatase inhibitors, through a planned process rather than a series of disconnected appointments.
Specialty breast cancer care centres are more likely to provide structured survivorship services than large general hospitals, simply because survivorship planning is a core function of their practice rather than an administrative afterthought. When breast cancer treatment ends, the relationship with a dedicated breast oncology centre does not. That continuity is one of the clearest arguments for choosing a specialist cancer hospital for your breast cancer care in Hyderabad.
Questions to Ask Before You Commit to Any Hospital
The consultation is not just a briefing where information flows in one direction. It is an opportunity to evaluate the hospital, the surgeon, and the team as much as it is an opportunity to receive a diagnosis and treatment plan. Most patients don’t exercise this right. The ones who do get better information, make better decisions, and are less likely to discover gaps in their care after treatment has already begun. For a useful checklist you can bring to the consultation, see questions to ask your doctor about breast cancer.
Questions About Surgical Expertise and Case Volume
Ask the surgeon directly: what specific surgical options are available for my diagnosis and why is one being recommended over another? How many breast surgeries does the operating surgeon perform per year, and what proportion of their practice is breast oncology specifically? Is oncoplastic or reconstructive surgery performed by the same team that does the cancer surgery, or is it referred to a different department or facility? Is sentinel node biopsy performed as standard for eligible patients, and who performs it?
The answers tell you whether the surgeon is comfortable with the full range of breast oncology surgical options or is more at home with a narrower set of procedures. A surgeon who hesitates or deflects on caseload questions is providing you with information as much as one who answers directly.
Questions About Treatment Protocols and Tumour Board Review
Will my case be reviewed by a multidisciplinary tumour board before the treatment plan is finalised, or will the plan be set by a single specialist? What receptor testing and molecular profiling will be conducted on my biopsy sample, and when will those results be available? Is targeted therapy available if my HER2 status requires it, and is the oncology pharmacy equipped to administer it? If neoadjuvant chemotherapy is recommended, what is the plan for reassessment before surgery, and how will response be measured?
These questions are not confrontational. They are the right questions for any patient entering a cancer treatment programme. A hospital with strong clinical systems answers them clearly, with specifics. A hospital without those systems often answers vaguely, with reassurances that do not address what was asked.
Questions About Cost, Timeline, and Support
Ask for a complete written estimate of the planned treatment cost, including what is and is not included in the quoted figure. Which government schemes or insurance networks does the hospital work with, and is there staff who can help navigate the claims process? Is there a patient coordinator or navigator you can contact throughout treatment for non-emergency questions and appointment coordination? How soon can treatment begin after registration, and what is the realistic timeline from first consultation to first treatment?
Hospitals that have thought seriously about the patient experience answer these questions with a process: they direct you to a financial counsellor, they give you a coordinator’s contact, they produce a timeline. Hospitals that have not built these systems give you a price and a name and leave the rest to you. The difference matters enormously across a treatment journey that may span six to eighteen months.
Make the Decision with a Clear Framework
Choosing the right breast cancer treatment hospital in Hyderabad is not about picking the biggest name or the most prominent location. It is about matching your specific diagnosis and stage to a hospital with the right surgical depth and team structure, and enough infrastructure to carry you through the full treatment arc, from the day you walk in to years after treatment ends.
Asvins Specialty Hospitals is built around exactly that model: a dedicated cancer specialist centre where breast surgery and gynae oncology are led by senior specialists, with Dr. G. Suryanarayana Raju’s four decades of focused surgical oncology experience, including his founding role at NIMS’s Surgical Oncology Department, as the clinical foundation. This is not a general hospital treating everything from orthopaedics to cardiology with cancer as one item on a long list. It is a hospital designed around the kind of concentrated, senior-led cancer care that patients travel specifically to access.
The next step is concrete. Bring your biopsy report, imaging CDs, and receptor status results to a specialist consultation at a dedicated breast oncology centre in Hyderabad. Ask the questions in this guide. Verify the tumour board process, the surgical team’s case volume, and the support services before you agree to a treatment plan. Don’t settle for a plan you don’t fully understand or a hospital that can’t answer your direct questions clearly. You are entitled to that clarity, and the right hospital will give it to you.
